Feb 24, 2023• Proven solutions
To celebrate its 10th anniversary, Facebook recently launched a Look Back Page. If you visit that page, Facebook's algorithm will auto-generate a video of your profile history. It will show the year you joined Facebook, your most-liked photos, statuses with the most engagement, accompanied with a standard piece of music.
It's pretty cool. But unfortunately, Facebook’s choice of pictures isn't. You may have to see some embarrassing old photos, or status updates that were funny at the time. In that case, you need to select the pictures of your choice, right?
The good new is that, Facebook has introduced a new editor now, which lets you choose your favorite images for the video. To edit the Look Back video, simply hit the "Edit" button on the top right corner of the Look Back page. Then un-check the photos and updates you don't want in your video, and check the ones that you want include. Once you're done, click the green "Share Your Movie" button at the top of the page.
Now you've selected the image you like. But what if the result is still disappointing? Don't worry! Here I'll introduce you a more powerful video editing tool to edit and enrich your Facebook Look Back video. Read on to get more information.

To edit the Look Back video, you should first download it. Then click "Import" to add it to the video editor, or drag and drop files to the User's Album. It will be displayed in thumbnail in the album and you can preview it on the right viewing window. Then place the Look Back video on the timeline.
To share the unforgettable moments in Look Back video, adding texts is a good idea. To do this, switch to Text tab and you'll see various texts templates on the left panel. Choose your favorite one and place it on the Timeline. Then the text thumbnail with a leading letter "T" will appear on the timeline. Double click it to type your texts in the box and select the font, color, animation, etc. Hit "Return" to confirm the settings and go back to the primary window.
Double click it to type your texts in the box and select the font, color, animation, etc. Hit "Return" to confirm the settings and go back to the primary window.
To adjust the background music of Look Back video, double click the video on the Timeline. In the pop up editing panel, switch to Audio column and change the Speed, Volume, Pitch of the audio file or add the Fade in/out effect as you like.
If you don't like the original background music of your Look Back video, just replace it and add a new one. To do this, right click the video and select the "Audio Detach" option. Then the background music will immediately be separated and appear on the music timeline. You can easily delete it and add a new one.
Wondershare Filmora (originally Wondershare Video Editor) can help you make your video wonderful and special by applying various elements. To apply some advanced effects, right click the video and select the "Power Tool" option from the pops up menu, or hit the "Power Tool" button above the timeline to enter the Power Tool window. Here you are provided tilt shift, mosaic, face off and jump cut at beats.
To apply some advanced effects, right click the video and select the "Power Tool" option from the pops up menu, or hit the "Power Tool" button above the timeline to enter the Power Tool window. Here you are provided tilt shift, mosaic, face off and jump cut at beats.
When everything is ready, click "Create" to save or share your videos in different ways:
Liza Brown
Liza Brown is a writer and a lover of all things video.
Follow @Liza Brown
Thank you for your comment. We will review it within few days.
Facebook mashes together timeline photos and posts for your “Look Back” video. But if you don’t like what the default algorithm selects, it can be edited.
The Facebook Look Back video is the social network’s gift for its users to celebrate its 10th birthday which was on February 4. Basically it mashes together the photos and posts from your timeline with generic background music — creating a one minute video. But there’s also basic editing tools to make it more how you like it. Here’s a look at how to use them.
Facebook’s Look Back feature generates a video for each user, showing what it thinks his or her best moments on the social network have been so far. Or, if you like, what Facebook’s script generates for the video.
That includes the moment you joined Facebook, your most liked posts, and shared photos. If you’re a user that uses your Facebook profile is a chronicle life moments — the default results can be impressive. If you’re into posting cat pictures, your Look Back movie will probably show your collection of felines.
If you’re a user that uses your Facebook profile is a chronicle life moments — the default results can be impressive. If you’re into posting cat pictures, your Look Back movie will probably show your collection of felines.
You can find your own Facebook Look Back movie here (you need to be logged in) and you can share the movie to your friends. The feature, which is signed by Mark Zuckerberg and the Facebook Team, has proved to be quite popular among users and tons of such movies have flooded Facebook timelines in the last few days.
There was even a grieving father who took to YouTube to ask Facebook to give him his deceased son’s video. His request was shared by thousands of people around the world and Facebook decided to grant him his wish.
While that’s all nice, there have been users complaining about wanting more control over what’s in their video. And Facebook answered the call. Editing what’s in your video is straight-forward and easy. Here’s how it works.
Start by going to your Look Back video; click the Edit button next to Share Your Movie. Scroll down to edit the Your First Moments section. If you don’t like what Facebook has picked, you can choose three other images that you find more appealing.
Next, you can select four of your Most Liked Posts for your video out of the list Facebook provides you with. Every time you change something, you can go back up to your video and preview your edits.
Uploaded Photos is the third section of the video you can play with. In this case, you can pick nine photos that you find suitable.
Last but not least, you can also edit the grid of photos which appears at the end of your video. This is the part where the biggest amount of work is required – no less than 39 photos need to be chosen.
Once you’re done, don’t forget to Share Your Movie. I couldn’t find a button which saves edits, so I think this is the only way to do so. However, if you don’t want the rest of the world to see it, you can always only share it with yourself, like I did in the screenshot below.
However, if you don’t want the rest of the world to see it, you can always only share it with yourself, like I did in the screenshot below.
If you’ve shared your movie before, you’ll notice that the Share Your Movie button now has Update on it.
You’ll get a small notification when your edits are done. The editor is basic and only allows for some simple tweaks, but it’s easy to use. Hopefully Facebook adds more editing features so you can pick your own music and maybe put short video spots in it…anyway, it’s amazing how such a simple thing is pleasing so many users.
Related Items:Facebook
Primary immunodeficiency (PID) was previously considered a fairly rare disease. However, with the development of diagnostics and screenings, it has been noticed that impaired immunity due to mutations in genes occurs in children and adults more often than expected. The average prevalence of this disease is 4 per 100 thousand. PID is dangerous because any infection, especially in a severe form of the disease, can lead to tragic consequences. Often, the first infection in the life of young patients becomes the last. However, if such patients are treated in time, they can lead a normal life.
The average prevalence of this disease is 4 per 100 thousand. PID is dangerous because any infection, especially in a severe form of the disease, can lead to tragic consequences. Often, the first infection in the life of young patients becomes the last. However, if such patients are treated in time, they can lead a normal life.
That is why many countries have launched neonatal screening for primary immunodeficiencies. Ekaterina Polyakova, Head of the Laboratory of Genetic Biotechnologies at the Republican Scientific and Practical Center, spoke about how things are going with this in Belarus.
"We also proposed to organize this work as a pilot project to be held in Minsk. The idea of screening was supported by Anzhelika Solntseva, Director of the Republican Scientific and Practical Center for Pediatric Oncology, Hematology and Immunology, and then by the Health Committee of the Minsk City Executive Committee. We believe that we will get good results and show the country that this is an effective method that can be applied throughout the country," said Ekaterina Polyakova.
Screening starts on April 1, it involves the study of TREC and KREC circular DNA structures, which are formed as a by-product of the formation of specific receptors for T- and B-lymphocytes. A decrease in the level of "tracks" and "cracks" indirectly indicates lymphopenia and deficiency of the T- and/or B-cell link of immunity, which accompanies a number of immunodeficiency states.
"Our center has developed its own diagnostic method. Many studies have been conducted, including retrospective material in children with primary immunodeficiencies. The method has shown 100% efficiency and 100% diagnostic sensitivity. The test allows you to detect violations of the T- or B-cell immunity", - said the head of the laboratory. Moreover, one of the Belarusian companies is working on the creation of an appropriate test system, which will be much more convenient to use.
According to Ekaterina Polyakova, it is important to identify primary immunodeficiencies in a timely manner. Especially dangerous is severe combined immune deficiency, which leads to severe illness, and in the absence of pathogenetic therapy, death in the first year of life.
Especially dangerous is severe combined immune deficiency, which leads to severe illness, and in the absence of pathogenetic therapy, death in the first year of life.
As explained by the head of the laboratory, children with this type of PID are usually born healthy, and it is impossible to determine the presence of primary immunodeficiency in the maternity hospital. It can be suspected only when the kids begin to get sick often and seriously, in some cases this leads to the death of the child. Screening, carried out in the first days after birth, allows you to reliably establish the presence or absence of the disease and, if necessary, start treatment.
"If we identify at least one child with lymphopenia per 1,000 examined, this will already be a good result. He can be saved in time if hematopoietic stem cell transplantation is carried out in the first six months of life. According to world data, its effectiveness is 95% in regarding the five-year survival rate," said Ekaterina Polyakova.
She explained that prognosis depends on the type of primary immunodeficiency. Hematopoietic stem cell transplantation is the main method of treatment, in particular for severe combined immunodeficiency. The bottom line is that with the help of chemotherapy and various methods of immunosuppression, the body's own cells are completely removed and donor cells that do not have breakdowns are populated by transplantation. When they engraft in the body of the recipient, the production of donor and own cells begins. As a result, the genetic defect disappears and the child develops normally.
In the case of immunodeficiency associated with a defect in the B-cell link of immunity, children often get sick. These are constant infections, pneumonia, bronchitis, etc. They are shown taking immunoglobulins.
The disease can manifest at different ages, but usually occurs in preschool. “The most dangerous for us is severe combined immunodeficiency, which we plan to detect during screening, since such children, as a rule, do not even live to be one year old,” said Ekaterina Polyakova.
If a child has lymphopenia, parents will be invited to the Republican Scientific and Practical Center and offered to undergo a second examination. If low TREC and KREC levels recur, the child will be referred for a consultation with an immunologist who is able to recognize primary immunodeficiency using additional immunological studies and prescribe the necessary treatment.
Newborns have been screened for many years in Belarus, for example, for phenylketonuria, hereditary metabolic disorders. In connection with neonatal screening for primary immunodeficiencies, no additional blood sampling and smears will be required: the drop of blood on filter paper that is taken from the heel of a child in the maternity hospital will be enough. As before, parents will be asked to sign an informed consent.
The study will also be useful when planning a pregnancy. It may be recommended to those couples who have had cases of death of children at birth or abortive miscarriages, which may be the result of primary immunodeficiencies. The study allows you to examine the defective gene and make a conclusion about whether the parents will pass it on to their unborn child or not, whether the child will be born healthy, sick, or simply be a carrier of this gene.
The study allows you to examine the defective gene and make a conclusion about whether the parents will pass it on to their unborn child or not, whether the child will be born healthy, sick, or simply be a carrier of this gene.
With information about the presence of disorders in a child still in the womb, doctors will be ready to perform an early hematopoietic stem cell transplant or prescribe supportive immunoglobulin therapy. Thanks to this, the child will be able to live a normal life.
BELTA.-0-
LISTEN TO THE RECORDING OF THE WEBINAR
Moderator Georgy Ignatiev at the beginning of the webinar “hung up” the question of why today, with good vaccination coverage and high-quality diagnostic tools, the measles virus is still with us.
The first speaker was Anna Nozdrach Yeva from the National Research Center for Epidemiology and Microbiology named after N.F. Gamaleya with a report on modern measles epidemiology. She began her report with statistics: in the early 2000s, the number of diseases significantly decreased - if thousands of people per 100,000 of the population used to get sick, now the incidence has dropped to 2-3 people per 1,000 of the population. But since 2010, the measles situation around the world has become unstable, recessions have alternated with ups, and in 2017–2019The incidence has been increasing throughout the world over the years. The largest contribution was made by the countries of Africa, the Middle East and the European region. By 2020, against the background of the coronavirus pandemic and restrictive measures, the incidence of measles began to decline again.
She began her report with statistics: in the early 2000s, the number of diseases significantly decreased - if thousands of people per 100,000 of the population used to get sick, now the incidence has dropped to 2-3 people per 1,000 of the population. But since 2010, the measles situation around the world has become unstable, recessions have alternated with ups, and in 2017–2019The incidence has been increasing throughout the world over the years. The largest contribution was made by the countries of Africa, the Middle East and the European region. By 2020, against the background of the coronavirus pandemic and restrictive measures, the incidence of measles began to decline again.
But the researchers noted that this well-being is largely imaginary. In 2021, the sources of infection remained in Africa and the Middle East, and as soon as restrictive measures became more localized in 2022, measles began to spread around the world again.
Nozdracheva and colleagues analyzed the statistics of infections and vaccinations in different countries of the world in recent years to compare vaccination coverage and incidence rates. To the researchers' surprise, there was no correlation. For example, in the United States, where coverage was not the highest (91.7% of the population received the first dose, and 87.5% received the second dose), the incidence was one of the lowest - 0.39 cases per 1000. And in the post-Soviet countries, where vaccination coverage exceeded 98%, the incidence was high and very high - from 2.1 people per 1000 to 71.8 people per 1000. However, there were more unvaccinated cases than vaccinated. According to 2019 data–2020 for different countries, in some regions the highest incidence is observed among children under 10 years old, although it is they who should be protected by the first vaccine they receive in a year.
To the researchers' surprise, there was no correlation. For example, in the United States, where coverage was not the highest (91.7% of the population received the first dose, and 87.5% received the second dose), the incidence was one of the lowest - 0.39 cases per 1000. And in the post-Soviet countries, where vaccination coverage exceeded 98%, the incidence was high and very high - from 2.1 people per 1000 to 71.8 people per 1000. However, there were more unvaccinated cases than vaccinated. According to 2019 data–2020 for different countries, in some regions the highest incidence is observed among children under 10 years old, although it is they who should be protected by the first vaccine they receive in a year.
Then the speaker spoke about the situation with measles in Russia. Until 2019, the incidence increased, in 2019 it reached a maximum and then decreased. At the same time, vaccination coverage of the population has been very high all this time - for the second vaccine, which is given in adulthood, it is 96% and higher since 2013. Nevertheless, a retrospective epidemiological analysis showed that Russia is an epidemically disadvantaged region in terms of measles. The incidence is growing against the backdrop of high vaccination coverage, it is growing among children, the number of foci of infection is increasing, as well as the number of medical workers documented vaccinated among those with measles. In 2023, there were several large-scale outbreaks of measles, the largest was in the Novosibirsk region, 9 people fell ill there5 people - 65 adults and 30 children. The source was unvaccinated people who came from a holiday in Thailand. Of the 40 people in the epidemic focus at the place of residence, only 19 were vaccinated. This situation arose primarily because of the parents' refusal to vaccinate their children. As a result, Rospotrebnadzor announced the start of clean-up immunization on April 3 - vaccination of unvaccinated and once vaccinated, as well as adults and children who did not have measles.
Nevertheless, a retrospective epidemiological analysis showed that Russia is an epidemically disadvantaged region in terms of measles. The incidence is growing against the backdrop of high vaccination coverage, it is growing among children, the number of foci of infection is increasing, as well as the number of medical workers documented vaccinated among those with measles. In 2023, there were several large-scale outbreaks of measles, the largest was in the Novosibirsk region, 9 people fell ill there5 people - 65 adults and 30 children. The source was unvaccinated people who came from a holiday in Thailand. Of the 40 people in the epidemic focus at the place of residence, only 19 were vaccinated. This situation arose primarily because of the parents' refusal to vaccinate their children. As a result, Rospotrebnadzor announced the start of clean-up immunization on April 3 - vaccination of unvaccinated and once vaccinated, as well as adults and children who did not have measles.
Nozdracheva and colleagues conducted a serological study of different age groups to find out if they had antibodies to the measles virus.![]() The proportion of seropositive in different age groups was about 75%, and 61.5% among children. Among medical workers it is higher - about 93%. At the same time, there were more people with immunity in the age group over 40. The incidence in older age groups was significantly lower, children were the most sick.
The proportion of seropositive in different age groups was about 75%, and 61.5% among children. Among medical workers it is higher - about 93%. At the same time, there were more people with immunity in the age group over 40. The incidence in older age groups was significantly lower, children were the most sick.
To find out why the incidence and proportion of seronegative individuals among the young population is increasing, scientists created a database of the results of sanitary and epidemiological investigations of measles cases and found that the actual coverage of the population with vaccines is lower than the declared statistics. The proportion of persons immune to the measles virus is less than the coverage of routine vaccination among people under 30-39years.
For the first time, it was possible to evaluate the results of anti-epidemic work in the outbreaks: emergency vaccination coverage among children was about 26%, and among adults - 40%. Vaccine refusals were 69.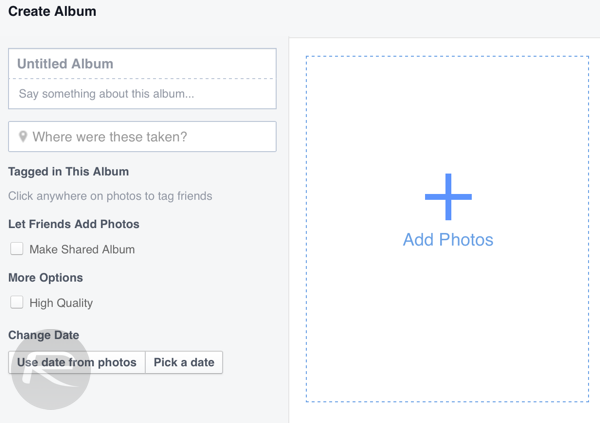 8% among children under two years of age and 42.3% among adults 20-35 years of age.
8% among children under two years of age and 42.3% among adults 20-35 years of age.
WHO data also show that vaccination coverage is declining around the world. Before the pandemic, it was 84%, but the pandemic itself and restrictive measures reduced coverage: people did not go to polyclinics once again, somewhere there were problems with the delivery of vaccines, and the forces of the medical institutions themselves were sent to fight the coronavirus.
Anna Nozdracheva noted that measles is a very highly contagious infection, and the level of population immunity should be about 95%. Its decrease by only 5% leads to an increase in the incidence among children by 3 times.
At the end, the speaker listed practical recommendations for increasing coverage: control of vaccination among children, clean-up vaccination, a clear definition of the list of medical exemptions from vaccination and the creation of an electronic vaccination passport. Anna also cited the Australian experience of fighting the anti-vaccination lobby as an example. There were outbreaks there, too, and the government began to withdraw disability benefits from those who contracted measles, because people were required to be vaccinated against it routinely. Opponents of vaccination were unhappy, but it helped. The measure is still in effect today.
There were outbreaks there, too, and the government began to withdraw disability benefits from those who contracted measles, because people were required to be vaccinated against it routinely. Opponents of vaccination were unhappy, but it helped. The measure is still in effect today.
Mikhail Kostinov from I.M. Sechenov posed an important question: is a third vaccination against measles necessary? In 1968, mass single vaccination of children from 12 months and other segments of the population began. In 1987, revaccination of children from 6 years of age and adults began, but then it was recommended only for people without immunity to measles. And only in 1997, mass revaccination of children older than 6 years began. Archival data from the Ministry of Health showed the same picture: up to 19In 1998, less than 50% were covered with revaccination, and only in 1998 the proportion of revaccinated children increased to 73.9% and began to grow - by 2003 it had grown to 95. 6%, and by 2007 - up to 97% and remained at this level until 2017 th.
6%, and by 2007 - up to 97% and remained at this level until 2017 th.
In 2018, Kostinov and colleagues assessed immunity to measles among the staff of a large medical facility. The proportion of seropositive individuals was 85%, the remaining 15% were seronegative. In order for population immunity to be maintained, the proportion of seronegative individuals should not exceed 7%. And again, as in the study discussed in the previous report, vaccination coverage on paper was higher than in reality.
An analysis of the results of other studies of measles immunity in medical workers in various regions of the Russian Federation showed that the proportion of seronegative individuals among them can reach 36% (data for 2016). In other words, doctors proved to be unsafe for patients and others. Among young people aged 19-23, the percentage of seronegatives was especially high - up to 38%. And only among people over 50 years old there were a sufficient number of people with immunity.
Further, Kostinov cited statistical data, according to which among children in 2001-2005 94% were revaccinated. At the same time, in 2018, among people 18-23 years old (these should be the same children), the proportion of seropositive was only 61%. According to the speaker, two doses of the vaccine cause a fragile immune response that does not persist throughout life.
The researchers also revealed gender differences in post-vaccination immunity: women from 40 to 50 years of age have less IgG antibodies than men of the same age. The proportion of seronegative women of this age may even be twice as high as the proportion of men. But after 55 years, the situation is reversed. Kostinov spoke about the results of their study of the immunity of women in labor of different ages in 2015. The proportion of seronegatives was the lowest among women aged 16 to 20 years - 10.3%, among women in labor 21-25 years old - 19.2% and the highest proportion - 25% - was among women from 26 to 35 years old. Only 11.8% of women from 36 to 43 years old were without immunity. At the same time, in Europe, there are much fewer women in labor without antibodies - 1.5% in Spain, 4.2% - in France.
Only 11.8% of women from 36 to 43 years old were without immunity. At the same time, in Europe, there are much fewer women in labor without antibodies - 1.5% in Spain, 4.2% - in France.
In this regard, Kostinov deduced risk groups for seronegativity to the measles virus: these are women from 26 to 35 years old and their newborns, as well as newborns of women with placental insufficiency and intrauterine infections during pregnancy (all this interferes with the migration of antibodies from mother to fetus). He suggests that women get vaccinated during preparation for pregnancy or immediately after childbirth, as well as vaccinate children earlier - up to a year, at 8-9months.
The speaker noted that many factors influence the formation of immunity after vaccination. For example, children who often suffer from SARS do not develop such high immunity - a year after vaccination, the proportion of seronegative among them can reach 30%.
At the same time, there are fewer contraindications to vaccination than is commonly believed. Among them are severe forms of allergy to aminoglycosides (but not allergies in general), primary immunodeficiencies, severe reactions and pregnancy. Among the false contraindications, Mikhail noted epilepsy, congenital malformations, asthma, eczema, dysbacteriosis, immunosuppressive therapy, and systemic connective tissue diseases. Pathologies make the body more vulnerable, and this is more of an additional reason to get vaccinated.
Among them are severe forms of allergy to aminoglycosides (but not allergies in general), primary immunodeficiencies, severe reactions and pregnancy. Among the false contraindications, Mikhail noted epilepsy, congenital malformations, asthma, eczema, dysbacteriosis, immunosuppressive therapy, and systemic connective tissue diseases. Pathologies make the body more vulnerable, and this is more of an additional reason to get vaccinated.
Kostinov concluded that immunity to measles may decrease over time, and immunocompromised individuals should be vaccinated 1–2 times, regardless of previous infection, previous vaccinations, and antibody levels. In his opinion, the third dose may be necessary, and it can be given, for example, in high school - planned and massively.
Then Yana Eremushkina , Associate Professor of the Department of Infectious Diseases and Epidemiology of Moscow State Medical University named after AI Evdokimov, talked about how a clinician can diagnose measles and distinguish it from rubella and other diseases. Measles can be typical or atypical, mild or severe, and may be smooth or uneven. Recently, an atypical mitigated form of measles is often found in previously vaccinated people, but who have lost immunity. This flow is characterized by mild catarrhal phenomena, low or normal temperature, the rash is small and dim. There is also a severe hypertoxic form of measles, in which the temperature, on the contrary, is very high, toxicosis, acute cardiovascular insufficiency and meningoencephalitis are observed.
Measles can be typical or atypical, mild or severe, and may be smooth or uneven. Recently, an atypical mitigated form of measles is often found in previously vaccinated people, but who have lost immunity. This flow is characterized by mild catarrhal phenomena, low or normal temperature, the rash is small and dim. There is also a severe hypertoxic form of measles, in which the temperature, on the contrary, is very high, toxicosis, acute cardiovascular insufficiency and meningoencephalitis are observed.
The most common complications are bronchitis, pneumonia, false croup, severe conjunctivitis, keratitis, otitis, sinusitis. The measles virus depresses the immune system, so complications are not uncommon. However, immunosuppression causes remissions of other pathologies, and it has even been used before. In the 20-30s of the 20th century, doctors noticed that children with nephritis who had measles had a remission of the underlying disease. And when someone got sick in the departments, the children were deliberately allowed to contract measles. Now they don't do that anymore.
Now they don't do that anymore.
Against the background of a typical course of measles, patients develop cerebral symptoms - from a sharp headache to meningeal signs - stiff neck, positive symptoms of Kernig, Brudzinsky. It was also noted that the earlier meningeal symptoms occur in patients, the more severe the disease will be. Yana Eremushkina spoke about the case of two women with measles who developed meningoencephalitis, which was indicated only by altered behavioral reactions - the symptoms were implicit. One of the hospitalized patients did nude aerobics;
From 2004 to 2014, 101 patients with measles were under the supervision of Eremushkina and her colleagues in CIB No. 2 in Moscow, among them 55% were women, 57% were people from 20 to 29 years old, and another 34% were people from 30 to 39 years old, the rest are older or children. Most of the cases were correctly diagnosed before admission, but 15 people were admitted with a provisional diagnosis of rubella. Thus, the differential diagnosis of measles and rubella is important - especially in the catarrhal (initial) period, before the appearance of characteristic rashes. During this period, most people infected with measles have a violent catarrhal reaction - conjunctivitis, laryngitis, rhinitis, tracheitis, photophobia. Rubella is characterized by a milder clinical picture. Also in the catarrhal period with measles, severe intoxication and Koplik-Filatov-Belsky spots are not uncommon - whitish spots on the mucous membrane of the cheeks and gums, similar to plaque that cannot be removed. Moreover, it is not always a whitish coating, sometimes it is rough redness - a residual phenomenon. In addition, measles is characterized by a rough, papular rash that usually appears on the face and descends within 2-3 days, in contrast to rubella, which has a non-rough rash that spreads throughout the body rather quickly - usually within a day. And with rubella, the lymph nodes on the neck and neck increase.
Thus, the differential diagnosis of measles and rubella is important - especially in the catarrhal (initial) period, before the appearance of characteristic rashes. During this period, most people infected with measles have a violent catarrhal reaction - conjunctivitis, laryngitis, rhinitis, tracheitis, photophobia. Rubella is characterized by a milder clinical picture. Also in the catarrhal period with measles, severe intoxication and Koplik-Filatov-Belsky spots are not uncommon - whitish spots on the mucous membrane of the cheeks and gums, similar to plaque that cannot be removed. Moreover, it is not always a whitish coating, sometimes it is rough redness - a residual phenomenon. In addition, measles is characterized by a rough, papular rash that usually appears on the face and descends within 2-3 days, in contrast to rubella, which has a non-rough rash that spreads throughout the body rather quickly - usually within a day. And with rubella, the lymph nodes on the neck and neck increase.
In 16% of patients monitored by Yana Eremushkina and colleagues, with severe measles, diarrhea was observed, vomiting - in 6%, Koplik-Filatov-Belsky spots were in the majority - in 83% of cases. In one case, there were ulcerative lesions of the oral cavity. A third of the patients had bronchitis and alveolitis, that is, against the background of measles, an erroneous overdiagnosis of pneumonia is possible. In 5%, the rash did not appear in stages from top to bottom, but first on the abdomen, arms or legs, and then spread throughout the body.
An experienced clinician, the speaker believes, is likely to distinguish measles from other diseases based on clinical manifestations, before test results.
Eduard Agletdinov , Deputy General Director for Research at Vector-Best, spoke about the dynamic control of post-vaccination immunity to measles and rubella using the example of the staff of their enterprise and teams of other institutions. (View presentation in pdf. ) In 2022, researchers from Vector-Best checked the post-vaccination status of employees (more than 700 people) for various infections. Thus, among those vaccinated against smallpox, 54% lost humoral immunity (there is no information about cellular immunity). In 24% of those who had previously been vaccinated against measles, antibodies did not survive - these employees were recommended revaccination.
) In 2022, researchers from Vector-Best checked the post-vaccination status of employees (more than 700 people) for various infections. Thus, among those vaccinated against smallpox, 54% lost humoral immunity (there is no information about cellular immunity). In 24% of those who had previously been vaccinated against measles, antibodies did not survive - these employees were recommended revaccination.
In January 2023, employees of a medical institution contacted Vector-Best with a request to check their measles vaccination status. Among the 105 examined seronegatives, 11 turned out to be, all of them were vaccinated and observed their immune status in a month - 10 people had enough antibodies, and one of them did not have very many, he will continue to be monitored. Another health facility made the same request in January, and employees without measles immunity were also vaccinated. Two months later, 8 out of 9the person was immune.
The next part of the report was devoted to rubella. Eduard Agletdinov showed the results of a study of immunity to rubella among the Vector-Best team: about 8% had no antibodies at all, and 7% did not have enough. Moreover, the older a person was, the stronger his immunity was - by analogy with measles. Agletdinov also recalled TORCH infections (toxoplasma, rubella, cytomegalovirus, herpes), which are transmitted in utero and threaten the health of the fetus. Rubella among the TORCH complex pathogens has one of the highest teratogenic effects and easily crosses the placenta. And although using PCR diagnostics, the RNA of the virus from the nasopharynx can be determined as early as three weeks before the onset of symptoms, during the incubation period, it is not possible to test all women or even all pregnant women. It would be better if data on the immunological and vaccinal status of people were collected massively (eg in schools) and made available.
Eduard Agletdinov showed the results of a study of immunity to rubella among the Vector-Best team: about 8% had no antibodies at all, and 7% did not have enough. Moreover, the older a person was, the stronger his immunity was - by analogy with measles. Agletdinov also recalled TORCH infections (toxoplasma, rubella, cytomegalovirus, herpes), which are transmitted in utero and threaten the health of the fetus. Rubella among the TORCH complex pathogens has one of the highest teratogenic effects and easily crosses the placenta. And although using PCR diagnostics, the RNA of the virus from the nasopharynx can be determined as early as three weeks before the onset of symptoms, during the incubation period, it is not possible to test all women or even all pregnant women. It would be better if data on the immunological and vaccinal status of people were collected massively (eg in schools) and made available.
To determine immunity to rubella, Vector-Best has test systems for the detection of antibodies VectoRubella-IgG, VectoRubella-IgM and VectoRubella-IgG-avidity, which evaluates the quality of IgG antibodies. The avidity index indicates how long ago the infection occurred. If it is less than 50, then the infection happened less than three months ago, if from 50 to 70, then 3-5 months ago, if more than 70, then more than 5 months ago. In turn, an IgM-only test may be false positive, for example, in the presence of rheumatoid factor in the blood or in response to infection with parvovirus B19. Together, these tests can help pregnant women who contract rubella decide whether to terminate the pregnancy (because the risk to the baby depends on when the woman becomes infected).
The avidity index indicates how long ago the infection occurred. If it is less than 50, then the infection happened less than three months ago, if from 50 to 70, then 3-5 months ago, if more than 70, then more than 5 months ago. In turn, an IgM-only test may be false positive, for example, in the presence of rheumatoid factor in the blood or in response to infection with parvovirus B19. Together, these tests can help pregnant women who contract rubella decide whether to terminate the pregnancy (because the risk to the baby depends on when the woman becomes infected).
Then Agletdinov listed unresolved or unresolved issues of vaccinology. In addition to the fact that vaccination coverage has declined in recent years due to the pandemic, the situation is complicated by migration flows from countries where vaccination is even worse, as well as problems with determining the quality of antibodies. In order to create quantitative tests, you need an international standard, but so far, many tests use different units of measurement and their results are difficult to compare with each other. A separate problem is the assessment of cellular immunity, the speaker noted.
A separate problem is the assessment of cellular immunity, the speaker noted.
After the presentation, Agletdinov was asked if they were testing the avidity of measles antibodies. He said that in the laboratory they tried to do this, and such a kit can be developed, but he does not see the need - in the case of rubella, the timing of infection is very important, not so with measles. However, it could be useful for assessing post-vaccination immunity.
Webinar was completed by Anastasia Nosova from the Center for Strategic Planning and Management of Medical and Biological Health Risks of the FMBA of Russia. She talked about diagnosing measles using real-time PCR and ELISA to detect IgM antibodies.
ELISA is the most commonly used, with reagent kits available in two formats: based on the indirect method and the double sandwich method; the latter have higher sensitivity and specificity. The advantages of ELISA are low cost, no need for expensive equipment, analysis is done quickly. However, in the early stages of the disease - in the first three days after the onset of the rash - you can get false negative results, because IgM accumulates gradually and reaches a maximum only on the 7-10th day. Therefore, real-time PCR is better suited for diagnosing measles in the early stages – it can be used to detect the virus even a few days before the rash appears. In addition, PCR analysis allows the simultaneous detection of several pathogens, if necessary. Different types of samples are suitable for analysis—nasopharyngeal secretions, saliva, urine, serum, and whole blood—but keep in mind that the viral load in different body fluids changes in different ways during the course of the disease. It is best to use swabs from the nose and oropharynx.
However, in the early stages of the disease - in the first three days after the onset of the rash - you can get false negative results, because IgM accumulates gradually and reaches a maximum only on the 7-10th day. Therefore, real-time PCR is better suited for diagnosing measles in the early stages – it can be used to detect the virus even a few days before the rash appears. In addition, PCR analysis allows the simultaneous detection of several pathogens, if necessary. Different types of samples are suitable for analysis—nasopharyngeal secretions, saliva, urine, serum, and whole blood—but keep in mind that the viral load in different body fluids changes in different ways during the course of the disease. It is best to use swabs from the nose and oropharynx.
Two Chinese studies compared methods for diagnosing measles. One of them showed that in the first three days the diagnostic sensitivity of PCR reached 94%, and ELISA - only 56%. But from the 4th to the 28th day, the sensitivity of the ELISA increased to 88%.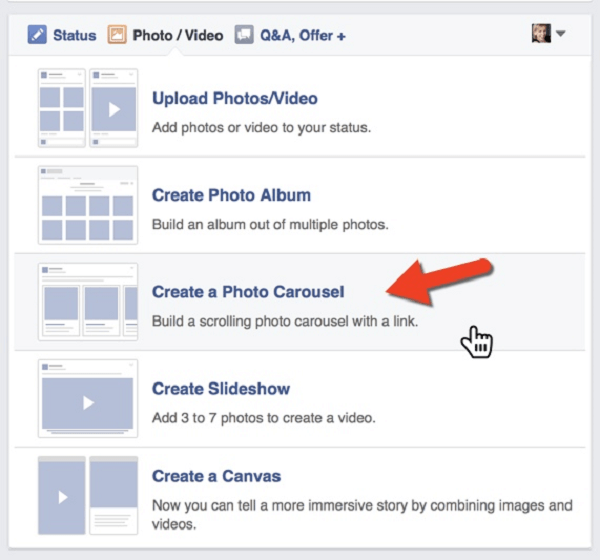 The second study showed that cases of measles without rash were better diagnosed by PCR, but even more effective was using both PCR and ELISA.
The second study showed that cases of measles without rash were better diagnosed by PCR, but even more effective was using both PCR and ELISA.
Then Nosova spoke about the reagent kits available on the market for both studies. Kits for ELISA are widely available and in different formats, and for PCR, despite the fact that many kits have been created, only one is registered in the Russian Federation - AmpliTest Measles. It allows the detection of measles virus RNA in nasal and oropharyngeal swabs and is designed for 50 determinations; analytical sensitivity — 10 3 GE/ml, analytical specificity - 100%.
In 2014, in the clinical guidelines for the epidemiological surveillance of measles in China, PCR was recommended as an additional method to routine ELISA. In the Russian recommendations, PCR is proposed to be used only to determine the genotype of the pathogen. In this regard, Anastasia notes that it is necessary to update the protocol for diagnosing measles and include PCR in it, expanding its use to confirm the diagnosis, ELISA results and testing of contact persons.
The speaker was asked how specific the Russian-made PCR kits are, how many genotypes they determine. Nosova replied that during the selection of primers, the nucleotide sequences of all genotypes are used, so the test systems capture all genotypes of the measles virus. But the emphasis during the specificity test is on the most common genotypes in the region - D8 and B3.
MODERATOR: Ignatiev Georgy Mikhailovich MD, professor, virologist
Nozdracheva Anna Valerievna N.F. Gamaleya" of the Ministry of Health of Russia
Eremushkina Yana Maratovna , candidate of medical sciences, associate professor; Department of Infectious Diseases and Epidemiology, Moscow State Medical and Dental University named after M.V. A.I. Evdokimov" of the Ministry of Health of Russia
Kostinov Mikhail Petrovich , Doctor of Medical Sciences, Professor, Head of the Laboratory of Vaccine Prevention and Immunotherapy of Allergic Diseases of the Federal State Budgetary Scientific Institution “Scientific Research Institute of Vaccines and Serums named after I./cdn.vox-cdn.com/uploads/chorus_asset/file/12803103/facebook-ios7-redesign.1419979915.jpg)